

Menopause marks the end of egg production, ovulation, and periods, but advances in medicine and assisted reproductive technology (ART) have made it possible for women in their late 40s and 50s to become mothers.
Still, this road is not without its complexities, medically, emotionally, and financially. In this guide, we help you prepare for it, addressing the main concern: Can you do IVF after menopause?
Can a woman get pregnant after menopause with IVF?
Yes, a woman can do IVF after menopause. Although menopause entails the end of natural fertility, any woman with a healthy uterus can conceive thanks to advances in reproductive medicine.
However, since the ovaries no longer release viable eggs, IVF after menopause is almost always done using donor eggs or embryos. You can also use your own eggs or embryos if they were preserved earlier in life. In this case, you would be pregnant with a biological child.

Source: Andre Furtado
The natural fertility decline
As you age, your fertility declines, but before it is completely gone, you go through the transition phase called perimenopause. It can begin several years before your final period, often in your 40s, but sometimes as early as your 30s.
During this time, your ovaries gradually produce less estrogen and progesterone, and levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) start to rise. These hormonal shifts lead to irregular ovulation, so in some cycles an egg is released, while in others it’s not. Although fertility is reduced, pregnancy can still happen naturally.

Source: Cottonbro studio
You officially reach menopause when 12 consecutive months have passed without a menstrual period. The average age is 51, but it can occur at any time between 40 and 55.
At this point, your ovaries stop releasing eggs altogether. LH and FSH levels remain high, while estrogen and progesterone stay low. Without ovulation, natural conception is impossible.
Then you get to postmenopause, the permanent state. Your hormone levels stay in the range that can’t trigger ovulation, but your uterus's function doesn’t stop in the same way your ovaries do. As long as it’s structurally healthy, it can still be prepared for pregnancy with the right hormonal support.
How successful is IVF after menopause?
The success of IVF after menopause depends on:
Egg quality: The fresher and healthier the eggs, the greater the chances of producing strong embryos.
Uterine receptivity: Hormone therapy can restore endometrial thickness and quality, but subtle differences in receptivity can still affect implantation.
Overall health: Age-related conditions, such as hypertension, diabetes, or cardiovascular disease, may influence pregnancy outcomes.
Medical approach: It’s essential to select a fertility clinic with experience and established protocols for treating women of your age and in your specific situation.
When high-quality donor eggs are used, postmenopausal women can achieve success rates similar to those of younger women using their own eggs.
IVF with donor eggs has high success rates (around 50–60% per cycle), regardless of the recipient parent’s age, because donor eggs come from a young, healthy, and thoroughly screened person, which eliminates age-related egg quality issues (chromosomal abnormalities) that can cause implantation failure and miscarriage.
Plus, success rates increase with every repeated cycle as presented below:
Cycle number | Success rate |
|---|---|
First cycle | Up to 59% |
Second cycle | 65% |
Third cycle | 89% |
For comparison, here is what IVF success rates look like when using your own eggs, according to SART:
Maternal age | Success rate |
|---|---|
Under 35 | ≅41.5% |
35 to 37 | ≅29.5% |
38 to 40 | ≅18.5% |
41 to 42 | ≅9% |
Over 42 | ≅3% |
Even with ideal eggs and expert medical care, success rates may still be slightly lower for postmenopausal women compared to younger parents due to age-related changes in the uterine tissue and general health.
Risks of IVF after menopause
Women who pursue IVF after menopause are more likely to have chronic health conditions due to advanced age, which can complicate both pregnancy and delivery. The most common issues that can appear are:
High blood pressure
Cesarean birth
Miscarriage or stillbirth
Premature birth or low birth weight
Personalized care, careful monitoring, and close collaboration with obstetric specialists experienced with high-risk pregnancies can minimize risks.
How can IVF work after menopause?
IVF after menopause looks more or less the same as conventional IVF. It starts with a consultation with a fertility specialist, who will assess your overall health, medical history, and uterine readiness. That often includes blood tests, pelvic ultrasounds, and, if necessary, more detailed imaging or cardiac evaluation to ensure pregnancy will be safe for you.

Source: Antoni Shkraba Studio
After this initial medical evaluation, you will go through the following four steps:
Hormonal preparation of the uterus
Choosing an egg donor and egg retrieval
Embryo development and screening
Embryo transfer and monitoring
1. Hormonal preparation of the uterus
Since the body doesn’t produce the estrogen and progesterone necessary to prepare the uterus for pregnancy, hormone replacement therapy (HRT) is a crucial first step in IVF after menopause.
The goal is to create a hormonal environment similar to that of a naturally fertile woman, allowing the uterus to support an embryo. Here’s how it works:
Estrogen stimulates the growth of the endometrial lining, making it thick and nutrient-rich.
Progesterone transforms this lining into a receptive state and maintains it during the early stages of pregnancy.
This treatment typically begins several weeks before embryo transfer. In some women, the uterus may have shrunk due to years of low hormone levels, so extended hormone therapy, sometimes spanning several months, can help rejuvenate it, restoring its size and function and improving the chances of successful implantation.
A healthy, receptive endometrial lining is one of the most important predictors of IVF success after menopause. Once the lining reaches the right thickness and quality, your doctor can schedule the embryo transfer.
2. Choosing an egg donor and egg retrieval
Unless you have preserved your own eggs or embryos, you will likely have to rely on eggs from external sources. Here is what the process typically looks like:
Donor selection: You can choose from a donor pool based on medical history, genetic screening, and personal characteristics.
Ovarian stimulation: The donor undergoes a cycle of fertility medications to produce multiple mature eggs.
Egg retrieval: Eggs are collected through a minor outpatient procedure performed under mild anesthesia, which typically takes about 30 minutes.
3. Embryo development
Once eggs have been retrieved, they are fertilized with sperm in a specialized laboratory in one of two ways:
Standard insemination: Sperm are placed around each egg in a culture dish.
Intracytoplasmic sperm injection: A single sperm is injected directly into an egg, often used when there are male-factor fertility concerns.
The embryos are then carefully cultured for 5–7 days, until they reach the blastocyst stage, when a distinction between cells that will become the placenta and those that will develop into a fetus is evident.

Source: Edward Jenner
During this time, embryologists track the division, shape, and development of embryonic cells, grading embryos based on their appearance and growth patterns.
Once the embryos reach the blastocyst stage, embryo genetic testing can be performed to screen for chromosomal abnormalities and inherited genetic disorders. It involves taking a few cells from each embryo, which is safe because the cells are removed from the trophectoderm (the part of the embryo that will develop into the placenta), while the inner cell mass (the part that will become the fetus) remains intact.
While you wait for the test results, your embryos are frozen and safely stored, which offers flexibility during the IVF timeline, allowing your uterus time to rest before implantation.
Here’s an overview of different preimplantation genetic testing (PGT) options:
Type of PGT | What it tests | Why it’s recommended |
|---|---|---|
PGT-A | Check for the correct number of chromosomes | Helps select embryos with the highest implantation potential and lowest risk of miscarriage |
PGT-M | Screens for specific inherited genetic diseases (e.g., cystic fibrosis, sickle cell disease, hemophilia, muscular dystrophy) | Recommended if the biological parents are known carriers of certain genetic conditions |
PGT-SR | Detects chromosomal rearrangements, such as translocations and inversions | Helpful if there are known chromosomal rearrangements in the parents |
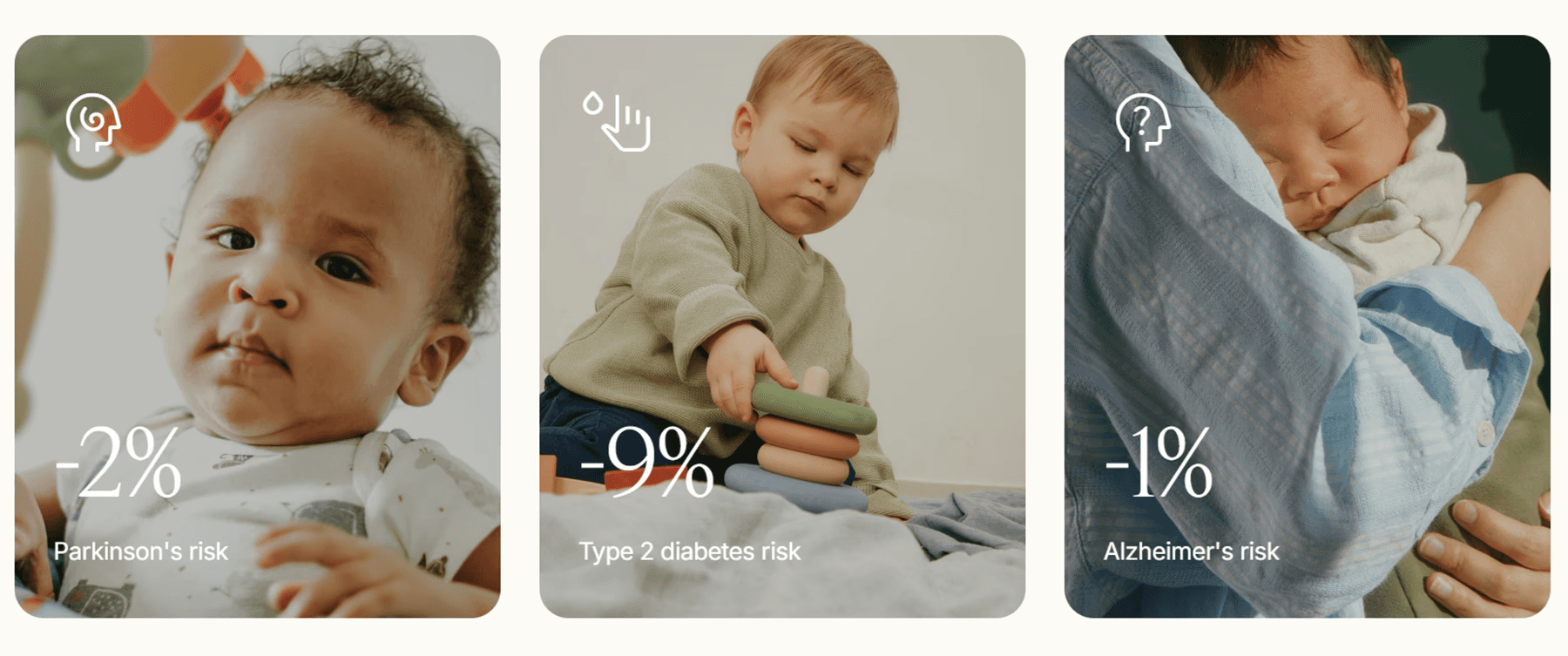
PGT-P | Evaluates embryos' potential risk for common chronic and late-onset conditions (e.g., heart disease, diabetes, Alzheimer’s) | Adds additional insights, allowing for the selection of embryos with potentially lower lifetime disease risk |
4. Embryo transfer and monitoring
Some clinics perform a mock transfer before the actual one. It is a quick practice that allows your doctor to measure the depth and angle of your uterus and identify any potential challenges. Mock transfers enable a smoother and faster procedure on the actual day. They are particularly valuable for women with uterine curvature or other anatomical variations.
When your uterine lining is at its peak thickness and quality, and the selected embryo is ready, it’s time for embryo transfer, a painless, non-surgical procedure done in a clinic setting.
Using ultrasound guidance, your doctor gently inserts a thin, flexible catheter through the cervix into the uterus to place the embryo in the optimal position for implantation.
The procedure usually takes only a few minutes, and you will likely resume normal activities immediately afterward, though many clinics recommend a brief period of rest.
After transfer, you will continue estrogen and progesterone therapy, in some cases until the end of the first trimester, to maintain a receptive uterine environment and support early pregnancy development.
The post-transfer phase includes blood tests (typically 9–14 days after transfer) to detect rising hCG levels and ultrasounds to confirm implantation and monitor early growth.
If pregnancy is confirmed, your care will transition to an obstetric team, though your fertility clinic may continue to support you during the early weeks.
Making informed choices during IVF after menopause
IVF involves many intricate stages, from preparing the uterus and selecting a donor to developing, testing, and transferring embryos. These stages require vital decision-making, and they must be carefully planned and executed to result in a healthy pregnancy and a live birth.
For women in or after menopause, this process can feel particularly overwhelming, especially when donor eggs or embryos might be necessary.
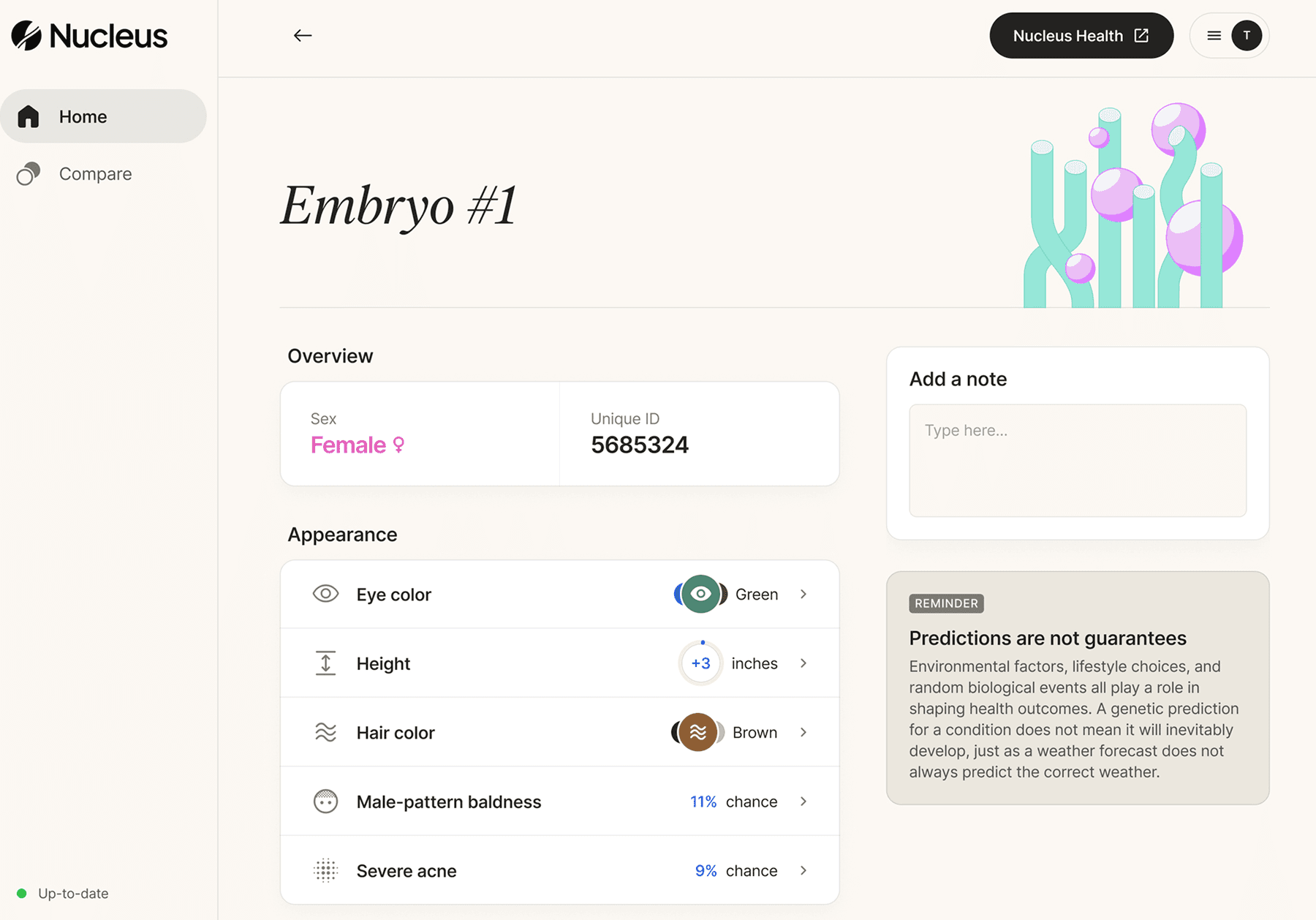
To streamline the process and focus on becoming a parent rather than dealing with every clinical detail alone, you can consider Nucleus IVF+, the first full-service IVF program that offers genetic optimization, testing, medication, and clinic networking with a human-centric approach.
How Nucleus IVF+ can help
Nucleus IVF+ combines advanced genetic analysis with compassionate, expert guidance to help you make the most informed reproductive choices, from the moment you decide to pursue IVF.
Nucleus IVF+ works with you to:
Guide clinic and donor selection: Choose a clinic with proven expertise in treating postmenopausal patients and access donor programs that meet the highest medical standards. Nucleus IVF+ can help you compare clinic protocols, evaluate donor profiles, and understand which options align best with your health and family goals.
Support genetic optimization: Through comprehensive carrier screening with Nucleus Preview, embryo genetic testing, and deeper analysis with our proprietary genetic optimization tool, Nucleus IVF+ helps identify embryos with the greatest implantation potential and the lowest genetic risk. This improves IVF outcomes and also supports decisions that prioritize the long-term health and well-being of your future child.
Provide ongoing expert support: From the initial consultation to embryo transfer, the Nucleus team offers clinical and emotional guidance, enabling you to make informed, evidence-based decisions at every milestone.
By helping you make thoughtful decisions at every step, we help you give your child the best possible start in life.
Book an onboarding call to get started.
You may also like…
Featured image source: Helena Lopes
















