

If you’re undergoing in vitro fertilization (IVF), the goal is clear: a healthy baby and the fewest possible cycles to get there. For many, this means using every available tool to increase their chances, including preimplantation genetic testing for aneuploidy (PGT-A) — a test that screens embryos for chromosome abnormalities before transfer.
PGT-A is often a standard part of care for patients over age 35, those with recurrent miscarriages, and couples who’ve experienced multiple failed IVF transfers. By identifying euploid embryos (embryos with the correct number of chromosomes), this test aims to increase implantation and live birth rates.
So, how often does PGT-A deliver on these goals? What percentage of embryos pass PGT-A testing? And, how well does the PGT-A testing success rate reflect an embryo’s potential?
This article will answer these questions by taking a closer look at:
What “success” means in the context of PGT-A
How often PGT-As lead to positive outcomes
Which factors influence PGT-A outcomes
Understanding PGT-A: How it works and what it aims to do
Unlike traditional embryo selection methods that rely on visual grading under a microscope, PGT-A helps count the chromosomes in each embryo to identify those with the correct number, called euploid embryos, before they are transferred to the uterus.
This test is typically performed at the blastocyst stage — five or six days after fertilization — via a biopsy. A few cells are gently removed from the outer layer of the blastocyst, called the trophectoderm, which will eventually become the placenta. These cells are then analyzed for chromosome abnormalities like extra or missing chromosomes, a condition known as aneuploidy.

Source: Edward Jenner
Embryos must inherit exactly 46 chromosomes — 23 from each parent — to develop normally. When this balance is disrupted, the embryo often can’t implant, stops developing, or results in miscarriage or serious genetic disorders such as Down syndrome and trisomy 18. Fully aneuploid embryos in which every cell has the wrong number of chromosomes miscarry in more than 86% of cases and almost never lead to a chromosomally normal live birth, with success rates below 2%.
PGT-A helps patients avoid becoming part of these grim statistics by screening out embryos with clear chromosome abnormalities before transfer, increasing the chances of a viable pregnancy and a healthy live birth.
Bonus reads: Learn more about PGT-A from the following guides:
PGT-A testing success rate: What does success mean in this context?
What defines PGT-A success depends on where the patient is in their IVF journey and what they or their doctor consider valuable progress. For many patients, it’s a live birth. For others, especially those of advanced maternal age, even reaching the point of having one euploid embryo is a meaningful milestone.
Most IVF patients measure PGT-A success based on four key metrics:
Finding a euploid embryo
Achieving implantation
Confirming a clinical pregnancy
Delivering a healthy baby
The table below explains each metric and how it’s typically measured and reported:
Success metric | Explanation | How success is tracked/reported |
Euploid embryo identified | Accurately spotting an embryo with the correct number of chromosomes | Reported per embryo tested, usually as a percentage of embryos that qualify as euploid |
Embryo implantation rate | The percentage of embryos transferred that successfully implant in the uterus | Tracked by clinical staff after embryo transfer, reported per transfer cycle |
Clinical pregnancy rate | The presence of a gestational sac with cardiac activity on ultrasound, indicating a viable pregnancy | Tracked by ultrasound scans, reported as a percentage of transfers leading to visible cardiac activity |
Live birth rate | The birth of a healthy baby — the gold-standard measure of PGT-A success | Reported per transfer or retrieval cycle; considered the most definitive outcome of an IVF treatment in general |
Tip: Before moving forward with PGT-A or any preimplantation genetic testing methods, have a discussion with your fertility specialist/counselor. They can help you define what success means for you, based on unique circumstances, such as age, medical history, or previous IVF experiences. Understanding success in this context will help you celebrate each milestone and make informed decisions throughout your journey.

Source: Pavel Danilyuk
3 real-world data points on the PGT-A testing success rate
Now that we’ve defined how PGT-A success is measured, let’s see how these outcomes hold up in real-world settings. We’ll review three key data points that highlight where PGT-A adds the most benefit — and where it may offer less advantage.
1. What percentage of embryos pass PGT-A testing?
PGT-A testing isn’t a guarantee that all embryos will qualify as euploid or chromosomally normal. The exact percentage of embryos that pass the test can vary based on multiple factors, including:
Patient age: Younger patients tend to have higher euploid rates.
Sperm health: Certain male infertility factors like abnormal morphology have been linked to aneuploidy.
Embryo quality: Embryos that appear healthy during visual grading are more likely to be chromosomally normal.
Studies report that roughly half of the embryos tested through PGT-A are euploid on average. One of the largest studies to date, analyzing over 24,000 embryos, puts this figure at 53.4%. Another smaller study across three independent genetic labs found an average of 44.3–44.8% euploid embryos, indicating slight variability depending on the lab and testing methodology.
The largest driver of variability is maternal age. In one trial reported by the American Society for Reproductive Medicine, as many as 69.8% of embryos were euploid — but the average patient age was only 29.1 years. As age increases, the proportion of euploid embryos tends to drop sharply due to a higher likelihood of errors during cell division.
The table below presents a general idea of the percentage of PGT-A normal embryos by age.
Age group | Percentage of euploid embryos |
Under 35 | 59–73% |
35–37 | 50–56% |
38–40 | 37–46% |
41–42 | 25–32% |
43–44 | 17–24% |
45 and over | 12–17% |
While these numbers may seem discouraging for patients of advanced maternal age, the latest fertility treatments and personalized care can make a huge difference in success rates.
You should also ask your clinic for additional tests like PGT-P to improve your chances of a healthy pregnancy. PGT-P is designed to screen embryos for polygenic disorders that depend on the cumulative effects of many genes associated with chronic and complex, late-onset conditions like type 2 diabetes and cancers.
Together, PGT-A and PGT-P can help you identify embryos with the lowest risk of chromosomal abnormality and predicted genetic risk. If your clinic doesn’t provide quality PGT-A or PGT-P testing, you can opt for comprehensive providers like LifeView.
2. What is the PGT-A testing success rate at different stages?
The next parameter is understanding how often PGT-A-tested embryos lead to successful outcomes — specifically, implantation, clinical pregnancy, and live birth rates.
These outcomes are best understood by comparing groups that underwent PGT-A (PGT-A treatment group) to those that didn’t (the control group). We examined comparisons from several clinical studies to better assess the true value of PGT-A beyond embryo selection, summarized below:
Success metric | PGT-A treatment group | Control group |
Implantation rate | 60–80% | 50–65% |
Clinical pregnancy rate | 41–51% | 37–46% |
Live birth rate | 40–66% | 39–48% |
The rates above represent average ranges. Individual outcomes can vary, with dramatic outliers in both directions. For example, one single-center study reported a live birth rate per embryo transfer as low as 11% without PGT-A, compared to 40.3% with PGT-A. Conversely, another large multicenter trial showed higher live birth rates in the control group (81.8%) than in the PGT-A group (77.2%).
These discrepancies highlight how PGT-A results aren’t universally predictive, and success depends heavily on individual factors. That’s why decisions around PGT-A should always be made on a case-by-case basis, after consultation with a fertility specialist.
3. What is the impact of maternal age on PGT-A outcomes?

Source: Amina Filkins
Age is widely considered the most significant factor in fertility, which holds true for PGT-A success rates as well. The table below summarizes the findings from different clinical studies that assessed IVF outcomes based on maternal age and the use of PGT-A:
Age group | Implantation rate* | Clinical pregnancy rate* | Live birth rate* |
Under 35 | 57–80% vs. 47–54% | 55–69% vs. 42–69% | 55–65% vs. 44%–69% |
35–37 | 57–60% vs. 36–45% | 57–70% vs. 37–62% | 50–59% vs. 37–57% |
38–40 | 57–64% vs. 25–35% | 44–63% vs. 35–45% | 44–44% vs. 24–36% |
41–42 | 51–60% vs. 17–25% | 47–58% vs. 15–30% | 47–53% vs. 16–23% |
43 and over | 47–57% vs. 7–9% | 42–58% vs. 5–20% | 44–53% vs. 12–23% |
*Outcomes with and without PGT-A
The overall evidence suggests that the benefit of PGT-A appears to increase with advancing maternal age. For women under 35, the evidence regarding the impact of PGT-A on IVF success rates is less conclusive, with some studies indicating no significant improvement.
This suggests that PGT-A may not provide a clear advantage for younger women in terms of increasing efficiency of IVF cycles, likely because they are more prone to producing euploid embryos. Still, it can be valuable for younger patients with a history of genetic conditions in the family or other risk factors, where pinpointing chromosomally normal embryos is essential.
Factors that influence PGT-A success rate
Besides maternal age, other notable variables that can impact PGT-A outcomes include:
Patient-specific variables
Embryo-related factors
Technical factors
1. Patient-specific variables

Source: Andreza Vasconcelos
The following patient-related factors can influence PGT-A success rates:
Paternal age: Advanced paternal age has been tied to some adverse outcomes, such as single-gene defects and stillbirth.
Body mass index (BMI): Elevated BMI has been linked to lower live birth rates, even when transferring chromosomally normal embryos.
Parental karyotype and genetic background: Parents with certain genetic changes in their chromosomes are more likely to produce embryos with aneuploidy.
Carrier screening can be a valuable step before IVF as it helps understand patient-specific genetic variables (to an extent) and determine testing options like PGT-P, PGT-A, or PGT-M.
Tip 👩❤️👨
You can go for comprehensive carrier screening options like Nucleus Preview to understand whether you or your partner carry inherited conditions that could impact embryo health.
Unlike standard genetic tests that analyze limited areas of your genome, Nucleus uses clinical-grade whole-genome sequencing to read nearly 100% of your DNA. With this level of insight — covering ~1,000 common conditions, traits, and rare diseases — you’ll have a clearer picture of your genetic health before making critical testing decisions during IVF. Order your Nucleus Preview kit today.

Bonus reads: Explore our dedicated guides to prenatal genetic testing and its pros and cons.
2. Embryo-related factors
When it comes to embryo-related factors, the quality of an embryo’s structure — particularly the inner cell mass (ICM) — is crucial. Euploid embryos with higher ICM grades have a greater likelihood of successful implantation and live births. The same goes for embryos that reach a fully expanded blastocyst stage by day 5 versus those that take longer, say, day-6 or day-7 embryos.
A Reddit user shared a clinic’s chart illustrating how embryo grading and developmental stages impact live birth success rates, which can help you better understand their correlation.
Mosaicism (when an embryo contains both normal and abnormal cells) is another important consideration. While some mosaic embryos can still lead to healthy live births, they generally have lower implantation rates and often require additional counseling and careful clinical judgment.
3. Technical factors
Technical factors cover everything that happens behind the scenes in the lab and clinic — from how embryos are biopsied to the technology used to analyze them. These elements directly affect the accuracy of any PGT results and the likelihood of a successful outcome. The most influential ones include:
Biopsy timing and technique: An experienced embryologist should perform the embryo biopsy at the blastocyst stage using proper technique to minimize harm to the embryo.
Laboratory environment: Culture media, incubator conditions, and handling protocols can all influence embryo development and, by extension, PGT-A outcomes.
Note that PGT-A is limited in scope — primarily focusing on detecting aneuploidy. You need to layer the analyses with PGT-P (and sometimes PGT-M and PGT-SR) to get a comprehensive genetic profile of each embryo. If you’re looking for high technical integrity, you can look into providers like LifeView that offer multiple PGT options or Orchid Health that offer whole-genome embryo testing.
Another great tool that can support you during IVF is Nucleus Embryo — a one-of-its-kind genetic optimization software. It translates your embryos’ PGT-P data into dozens of comparable insights about health conditions and traits affected by multiple genetic elements.
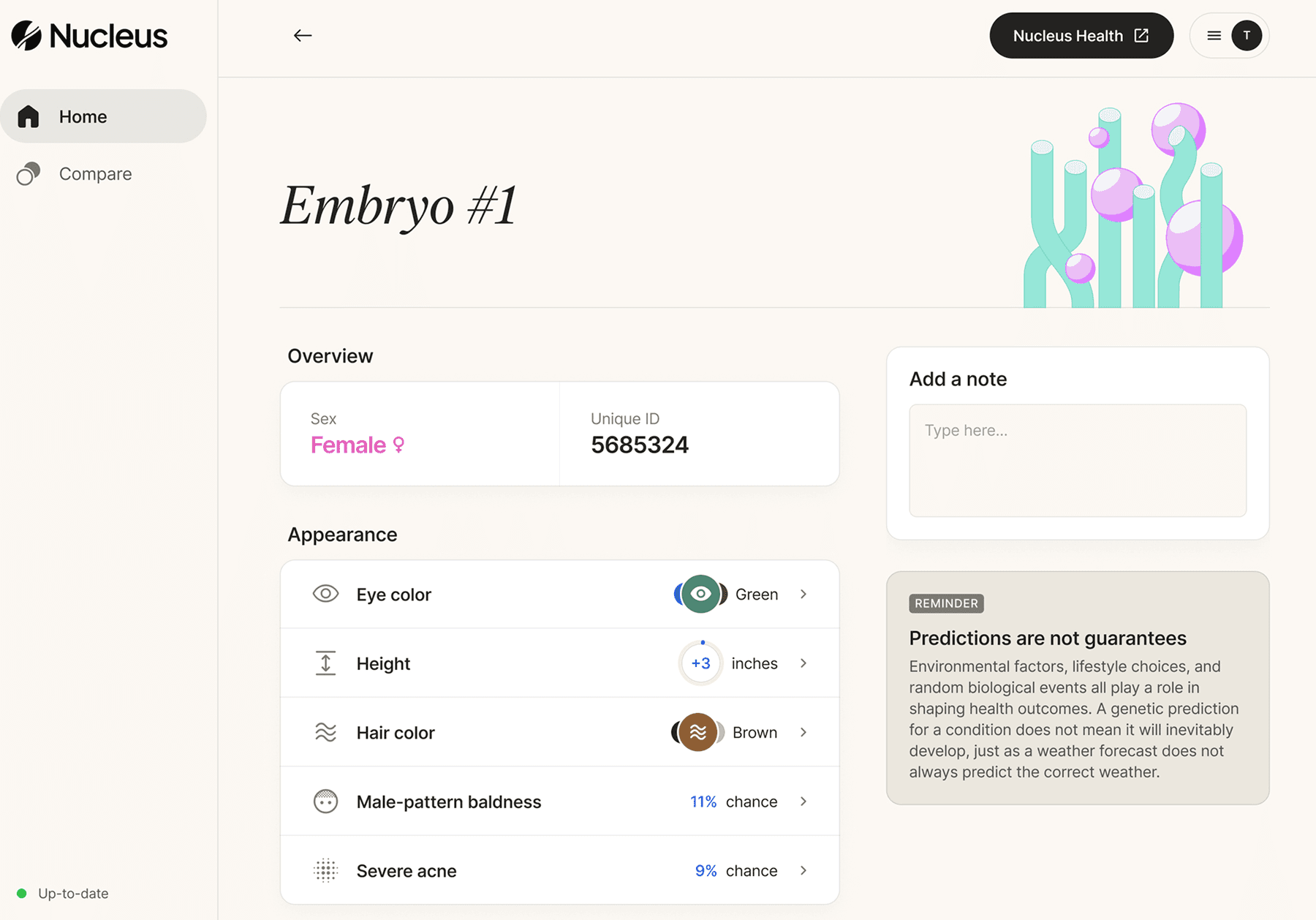
How Nucleus Embryo can help improve IVF outcomes
Nucleus Embryo is a genetic optimization software created specifically for couples undergoing IVF who want to take a health-first approach during embryo selection.
With Nucleus, you can use genetic insights to examine an embryo’s lifetime risk for developing complex, chronic, and late-onset conditions such as type 2 diabetes, heart disease, mental health and cognitive disorders, and more. These are conditions impacted by multiple genes that are best uncovered by PGT-P testing, which can be comfortably done alongside PGT-A.
Nucleus Embryo provides dozens of genetic insights per embryo, including:
Common and rare health conditions
Heart disease, ADHD, Alzheimer’s disease, and more
Traits
Eye color, height, left-handedness, and BMI, among others
Well-being indicators
Seasonal allergies, alcohol dependence, and more
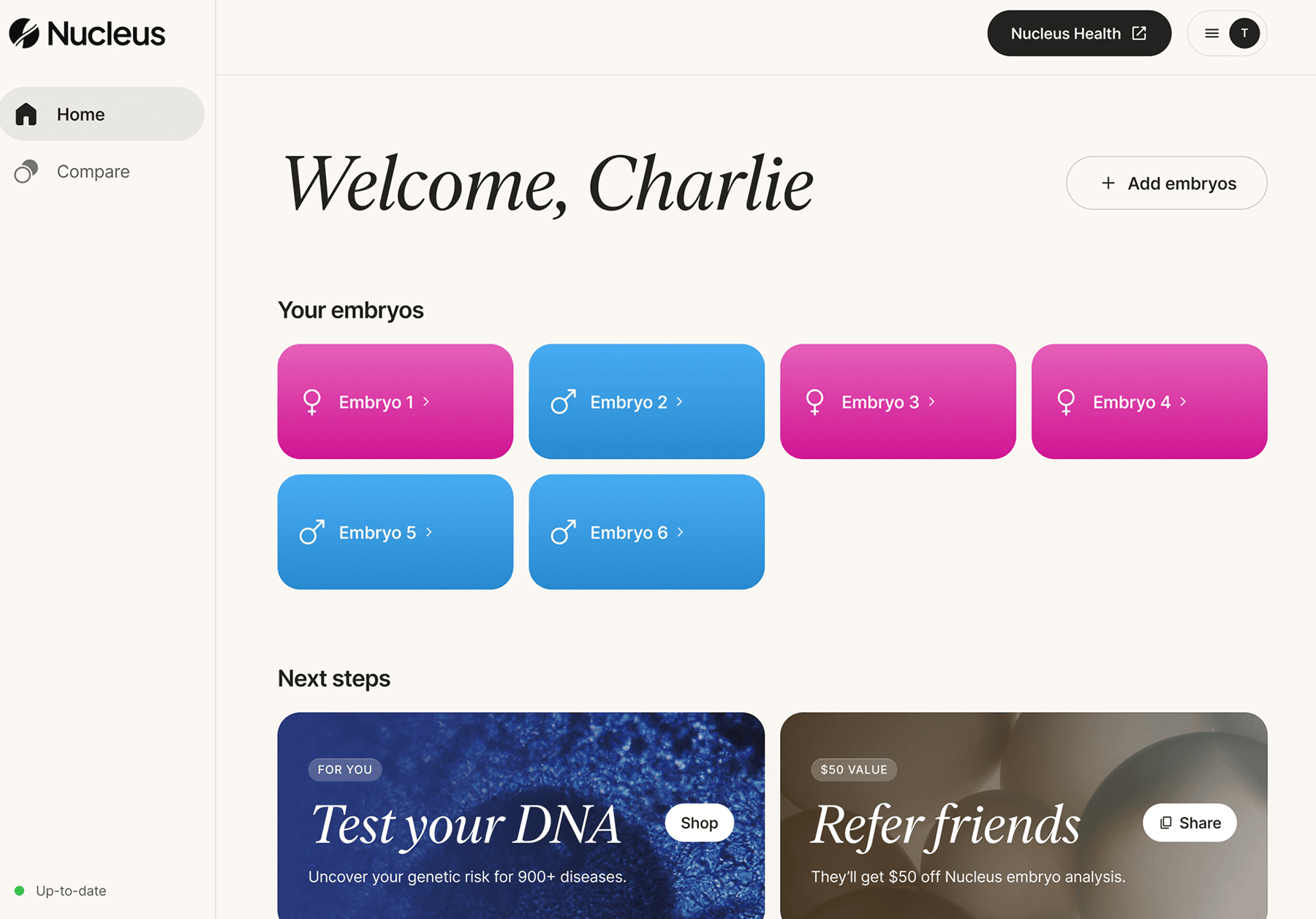
You can upload up to 20 embryos and sort, compare, and select them in a clean, intuitive dashboard. The platform is made for prospective parents, not scientists. It turns complex genetic data into meaningful insights that you and your partner can easily interpret.
The platform is HIPAA-compliant and follows the industry-best user privacy practices.
How credible is Nucleus Embryo
Nucleus Embryo is rooted in rigorous science and the latest developments in genetic technology. It’s designed to support individual autonomy, and not replace medical expertise. The goal is to empower you to make informed decisions with reduced emotional strain during the IVF process.
Remember that you need to ask your clinic for PGT-P during IVF genetic testing to make sure you can benefit from Nucleus’ genetic optimization tool. Here’s a quick overview of the next steps:
Ask your clinic for PGT-P testing with LifeView by Genomic Prediction
Sign up for Nucleus Embryo during or after you complete your IVF cycle
Request your embryos’ PGT-P DNA data from your clinic
Upload the data to Nucleus Embryo and analyze the embryo analysis report
Every child’s story starts somewhere — Nucleus helps you make the beginning stronger, smarter, and more intentional from a health perspective. You can fill out the form on this page to get started today.
Featured image source: RDNE Stock project










