

When you’re going through IVF, each embryo carries hope, fear, and the dream of a healthy baby. The path can be winding, and every decision feels critical, especially when it comes to choosing which embryos to transfer.
PGT-A testing, short for Preimplantation Genetic Testing for Aneuploidy, is becoming a common step in the IVF process. It offers valuable information about the chromosomal health of embryos, and it can help you make informed decisions during fertility treatment, as well as improve implantation rates and reduce the risk of miscarriage.
This guide explores what PGT-A test is for, how it works, and who benefits most from it. We’ll also break down its accuracy and limitations and explain how to interpret the results so you can gain more clarity and make more confident decisions.
What is PGT-A testing in IVF?
PGT-A (sometimes still referred to by its older name, PGS — Preimplantation Genetic Screening) is a screening tool used during IVF to examine whether embryos have the correct number of chromosomes. If they do, they are called euploid, but if abnormalities exist, they are called aneuploid.
PGT-A can help you and your medical team choose the most viable embryos for transfer by identifying which embryos are euploid. This can improve the chances of implantation, reduce the risk of miscarriage, and may shorten the overall time to pregnancy, especially in cases where only one embryo is transferred at a time.

Source: cottonbro studio
What does PGT-A test for?
Parents going through IVF face many big decisions and have many questions. PGT-A offers answers by identifying which embryos are most likely to lead to a healthy pregnancy and which may not develop at all.
Here’s an overview of the types of chromosomal issues PGT-A typically screens for:
Chromosomal issue | Examples and conditions |
Extra chromosomes (trisomies) |
|
Missing chromosomes (monosomies) |
|
Sex chromosome abnormalities |
|
Some PGT-A tests can also detect uniparental disomy (UPD), a condition where an embryo gets both copies of a chromosome, or part of a chromosome, from one parent, instead of one from each.
Most of the time, this doesn’t cause any problems, but sometimes, it can affect how certain genes work. If that happens, it can lead to health or developmental issues, such as:
Prader-Willi syndrome
Angelman syndrome
Beckwith-Wiedemann syndrome
Bonus read — See how PGT-A compares to prenatal tests:
How does the PGT-A test work?
The PGT-A test is designed to be minimally invasive, posing little to no risk to the embryo. Here’s how the procedure works:
Embryo development: The embryos are cultured in the lab for 5–6 days until they reach the blastocyst stage when the embryo has developed two cell groups — the inner cell mass (future fetus) and the trophectoderm (future placenta).
Trophectoderm biopsy: A small number of cells (usually 5–6) are removed from the trophectoderm (never from the part that will become the fetus) to minimize the risk to the embryo. These cells are expected to reflect the genetic makeup of the whole embryo, although this isn’t always guaranteed.
Embryo freezing: After the biopsy, the embryo is frozen and safely preserved until the PGT-A test is completed and a decision about transfer can be made.
Chromosomal analysis: The biopsied cells are sent to a genetics lab, where technicians count the number of chromosomes, examine their shape and structure, and identify missing or extra segments.
PGT-A results: A report is sent to your fertility clinic typically within 1–2 weeks.
Embryo selection and transfer: You choose the healthiest embryo(s) for frozen embryo transfer (FET). The embryo is thawed and transferred into the uterus when your body is ready. Any additional healthy embryos can be kept frozen.
Since PGT-A examines all 46 chromosomes, including the two X and Y sex chromosomes, the test also reveals the sex of the embryos (with over 98% accuracy). This information is routinely included in the PGT-A report and can be valuable if it is necessary to avoid certain sex-specific genetic disorders.

Source: Olia Danilevich
How accurate is PGT-A testing?
According to some sources, the accuracy of PGT-A is over 97%. Other sources show that the test correctly identifies most embryos with chromosomal issues about 84% of the time.
This implies that some healthy embryos may be wrongly labeled as abnormal — a false positive result. Studies suggest that about 40% of embryos flagged as abnormal may actually be viable.
False negatives — when an abnormal embryo is mistakenly labeled as normal — are also possible but less common. Depending on the study, rates of false negatives range from 0.1% to 23%.
That said, the overall chance of a misdiagnosis per embryo transfer is estimated to be around 0.2%. This means that two in 1,000 presumed euploid embryos are actually aneuploid and may have caused miscarriage or failed implantation.
Although today's PGT-A testing methods are highly accurate, it’s important to remember that this is a screening test, not a diagnostic one. Therefore, PGT-A can't guarantee a healthy baby, as there’s still a small chance of false positive or false negative results.
PGT-A helps identify embryos without chromosomal abnormalities, but it can’t rule out all genetic conditions or polygenic risks, such as those associated with heart disease, diabetes, or certain cancers.
💡Bonus tip
For many patients, PGT-A results are just the beginning. You may want deeper insights, especially if you need to choose between multiple healthy options. That’s where PGT-P — a genetic analysis for chronic and late-onset conditions, like heart disease, cancers, Alzheimer’s disease, and more — comes in.
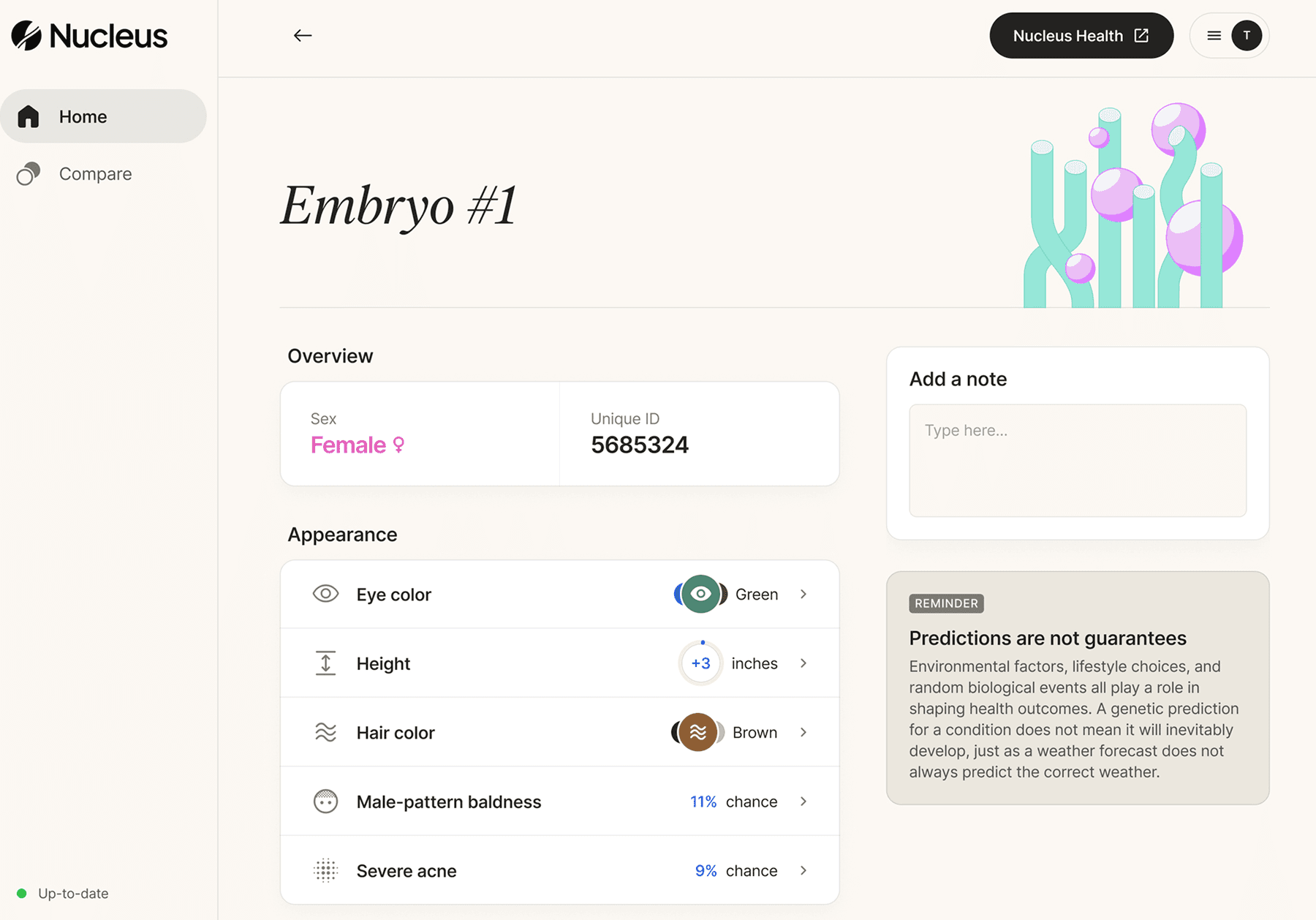
Tools like Nucleus Embryo can help you dive deeper into your PGT-P data to understand and select your embryos based on what matters most to you.
Each prediction is explained in clear, everyday language so you can understand your results without a science degree.
Get more clarity with Nucleus Embryo.

Interpreting PGT-A testing results
Getting your PGT-A report can feel overwhelming, but understanding the results can help you and your doctor make informed decisions about your next steps.
PGT-A results typically fall into one of four categories:
Euploid
Aneuploid
Mosaic
Inconclusive
We’ll explain each category in more detail in the sections below.
Euploid
If your embryo is marked euploid, it means it’s chromosomally normal, having the correct number of chromosomes — 23 pairs, or 46 in total. This includes:
22 pairs of autosomes, which carry most of the genetic information that determines traits like eye color, height, and more.
1 pair of sex chromosomes, which determine biological sex. Two X chromosomes (XX) indicate a genetically female embryo, and one X and one Y chromosome (XY) typically indicate a genetically male embryo.
This is considered the ideal result and gives the embryo the best chance of implanting and developing into a healthy baby.

Source: Pixabay
Aneuploid
An aneuploid embryo means there is an abnormal chromosome count — either too many or too few chromosomes.
Aneuploidy is one of the most common reasons why early pregnancies fail to progress. According to one study, embryos with clear signs of chromosomal issues (aneuploidy) have a very high chance of miscarriage (86.3%). Additionally, in 98% of cases, they don’t result in the birth of a chromosomally healthy baby.
In IVF, aneuploidy is surprisingly common — up to 50% of embryos tested with PGT-A are found to have chromosomal abnormalities. These abnormalities can prevent an embryo from implanting, increase the risk of miscarriage, or, in some cases, lead to serious genetic conditions, which is why aneuploid embryos are typically not transferred.
While that number may seem high, it’s completely normal and reflects a natural variation in embryo development, not a problem with the IVF process, the eggs, or the sperm.
Mosaic
Mosaicism happens when an embryo comprises a mix of both chromosomally normal (euploid) and abnormal (aneuploid) cells. About 15% of all embryos are mosaics.
However, it is possible that the tested sample doesn’t reflect the genetic makeup of the whole embryo. For example, the tested cells might appear normal, while some untested cells are abnormal and vice versa.
Because of this, mosaicism can lead to uncertain or potentially misleading PGT-A results, including false positives or false negatives.
Still, a mosaic embryo may be considered for transfer, especially if no euploid embryos are available and the patient chooses to move forward. A detailed consultation with a genetic counselor is often necessary in this case.
Mosaic embryos are assessed based on the proportion of abnormal cells and which chromosomes are affected. Doctors may recommend mosaic embryo transfer if the abnormal portion is low and involves chromosomes with less risk.
While transferring a mosaic embryo can lead to a healthy pregnancy, it does come with a higher risk of miscarriage and lower chances of success compared to euploid embryos.
Inconclusive
In some cases (about 5%), PGT-A testing does not return a conclusive result. This doesn’t mean something is wrong with your embryo or that it is unsuitable for transfer. It only means the lab couldn’t come to a confident conclusion.
This may happen due to:
Poor-quality DNA: Sometimes, embryos don’t develop well enough to yield usable samples. These embryos may have stopped growing before day 5–6 or had too few cells to biopsy.
Insufficient sample size: PGT-A typically requires 5–10 cells for analysis. If fewer cells are retrieved, the sample may not be sufficient for reliable testing.
Failed amplification: During testing, the DNA from the cells is copied (amplified) to produce enough material for analysis. If amplification fails, no result can be obtained.
Misinterpretation: If the sampled cells were not representative (e.g., all abnormal cells from a mostly normal embryo), results could be misleading, especially in suspected mosaic cases.
Technical issues during testing: Contamination with DNA from another source and errors during handling, shipping, or processing in the lab are rare but possible.
If you receive a “no result” PGT-A report, your healthcare provider may recommend repeating the test on another embryo or performing a second biopsy (if feasible). In some cases, you may need to undergo another IVF cycle to retrieve and fertilize new eggs.
How maternal age impacts PGT-A results
Chromosome abnormalities are a natural part of human reproduction, but they become more common as the mother ages. This is true whether conception happens naturally or through IVF.
As we age, the number of eggs retrieved during IVF cycles tends to decrease, and the chance that those eggs will lead to chromosomally normal embryos also decreases. This can affect how many embryos are suitable for transfer after PGT-A.

Source: Remembryo
While different studies may report different numbers, the table below shows PGT-A results by age and offers an average estimate of the chance of having an aneuploid embryo based on the age of the person providing the eggs:
Age of egg provider | Chance of aneuploidy |
Under 30 | 33% |
30–34 | 38% |
35–37 | 47% |
38–40 | 60% |
41–42 | 76% |
43 and older | 84% |
These figures are meant to help you understand general trends while remembering that everyone’s journey is unique. Some patients may have more or fewer normal embryos than average.
While statistics can offer helpful insights, they can also be challenging to interpret, especially concerning something as personal and complex as IVF outcomes. There are different factors at play, as shown in this Reddit comment:
Should you do PGT-A testing?
PGT-A is now the standard of care provided to almost anyone undergoing IVF as it helps understand embryo quality before transfer.
If there’s a known genetic disorder in the family or a chromosomal rearrangement, a different test, like PGT-M (for monogenic diseases) or PGT-SR (for structural rearrangements), may be more appropriate.
If you have a family history for a chronic condition like cancer, type 2 diabetes, heart disease, or Alzheimer’s disease, you can request an analysis known as PGT-P from your provider. PGT-P can offer insights into your future child’s risk for chronic and late-onset conditions — which adds more transparency to the embryo selection process.

Source: MART PRODUCTION
To help clarify the differences between these tests, here's a comparison to guide your decision-making process:
Test type | What it does | Who it is for |
PGT-A | Checks for the correct number of chromosomes |
|
PGT-M | Screens for a specific inherited disease caused by a single gene mutation (e.g., cystic fibrosis or Tay-Sachs) |
|
PGT-SR | Detects unbalanced chromosome changes due to translocations or other structural abnormalities |
|
PGT-P | Detects the likelihood of developing many complex diseases based on the genetic differences across multiple markers |
|
PGT-A, PGT-M, PGT-P, and PGT-SR only show part of the picture. While these tests help identify chromosomal abnormalities, monogenic disorders, or structural rearrangements, they don't offer insight into other genetic factors that could influence your baby’s health or future.
After PGT-P or whole-genome on your embryo files, Nucleus Embryo is a natural next step for parents who want a fuller picture of their embryo’s potential. While PGT-A focuses on viability and chromosome count, Nucleus dives deeper, analyzing what traditional screening can’t see.
The first genetic optimization software designed for IVF patients lets you analyze up to 20 embryos at once, screening for dozens of inherited conditions and providing insights into physical health, mental wellness, and more.
With clear reports and visual embryo comparison, Nucleus helps you feel more informed and ready to move forward.
Go beyond basic embryo viability: Choose Nucleus Embryo
For families with multiple embryos, choosing the right one can feel like guesswork. Nucleus Embryo helps decode deeper layers of genetic information, so you can have a clearer understanding of your options.
Nucleus Embryo provides valuable information, assessing your embryo's potential risks for dozens of chronic and late-onset conditions, as well as genetic predispositions for eye color, hair color, height, and more. As a one-of-its-kind genetic optimization tool, Nucleus helps translate your embryos’ genetic data into actionable insights. If you prioritize your future child’s long-term health and well-being, you’ll find the following Nucleus insights meaningful:
Health conditions: Heart disease, cancer risk, neurological health, women’s health conditions, ADHD, and depression
Well-being and more: Get markers for intelligence, mental health risks, and more
You can also gain insights into traits, such as height, eye and hair color, and other characteristics that may matter to you. Nucleus Embryo is designed to be parent-friendly with the help of an interactive dashboard that makes it easy to compare embryos side by side, as well as sort and filter them for a personalized view.
With Nucleus Embryo, you get more than just numbers — you can give your future children the best possible start in life.
How to start with Nucleus Embryo
Once your PGT results are ready, getting started with Nucleus Embryo is simple:
Ask your clinic for PGT-P testing with LifeView by Genomic Prediction
Sign up for Nucleus Embryo during or after you complete your IVF cycle
Request your embryos’ PGT-P DNA data from your clinic
Upload the data to Nucleus Embryo and analyze the embryo analysis report
Make confident, informed choices about your embryo transfer, grounded in science and tailored to your family’s future.
You may also like…
Explore more resources as you navigate through your IVF journey:
Featured image source: RDNE Stock project










