

For specific parent groups, the path to starting or growing a family comes with additional challenges to an already demanding IVF process. IVF surrogacy (the more common term for gestational surrogacy) helps overcome medical and practical barriers to having a baby associated with single-man parenting, same-sex parenting, or a woman’s inability to carry a pregnancy.
This guide clarifies how gestational or IVF surrogacy works so that you feel better prepared for this long and complex journey.
What is gestational surrogacy?
Gestational surrogacy is a family-building option in which another woman, called a gestational surrogate or gestational carrier (GC), carries and delivers a child on behalf of someone else. The individual or couple who plan to raise the child are called the intended parents. This type of surrogacy requires creating the embryo from the intended parents’ or donors’ genetic material, which is why it’s also called IVF surrogacy.
How does gestational surrogacy differ from traditional surrogacy?
Traditional surrogacy is a family-building arrangement where the surrogate uses her own egg to conceive, making her the biological mother of the baby. The intended parents provide the sperm or use a donor, while the surrogate carries the pregnancy to term. In most cases, at least one of the intended parents is genetically related to the baby.
Because the carrier is the biological parent, she has automatic parental rights at birth. To transfer custody, she must legally surrender those rights to the intended parents. In some states, this requires a formal adoption process. Traditional surrogacy is legally riskier and more complex because the surrogate’s consent is central, and in theory, it could be revoked. Paid surrogacy contracts could also be illegal in some states.

Source: RDNE stock project
In contrast, in gestational surrogacy, the GC has no genetic link to the baby since the pregnancy is conceived through the intended parents’ (or another donor's) egg and sperm. Courts are more likely to recognize the intended parent’s rights from the start, but state laws may vary.
The genetic connection in traditional surrogacy can create emotional complexity for both intended parents and the surrogate. Gestational surrogacy generally reduces these challenges. Still, clear communication, mutual expectations, and supportive counseling can help manage relationships and ensure a positive experience for everyone involved.
Does surrogacy always require IVF?
Gestational surrogacy without IVF isn’t possible because the surrogate doesn’t use her own eggs. An embryo is created in a lab using the egg and sperm from the intended parents or donors, and then transferred into the IVF surrogate’s uterus.
Traditional surrogacy can involve either IVF (in vitro fertilization) or IUI (intrauterine insemination) to transfer the sperm, since the surrogate’s own egg is used in conception.
Who is IVF surrogacy for?
IVF with a gestational carrier is an excellent option for individuals and couples who want to build a family but can’t carry a pregnancy themselves due to conditions such as:
Absence of a uterus (from birth or hysterectomy)
Uterine conditions (Asherman’s syndrome or congenital malformations)
Medical conditions, such as heart disease, kidney disease, or autoimmune disorder
Recurrent pregnancy loss or multiple failed IVF transfers despite good-quality embryos
Medications or treatments that could harm a developing fetus
For many LGBTQ+ families, IVF is the most accessible path to parenthood, since it enables using donor eggs, donor sperm, or a gestational surrogate to grow a family. Beneficiaries include:
Gay male couples using donor eggs and a gestational carrier
Two women may use one partner’s eggs with a gestational surrogate
Single men
Trans men and women whose bodies or medical treatments prevent pregnancy

Source: Kaboompics.com
The IVF surrogacy process in 6 steps
While the IVF process is typically the same for most parents, a few additional steps are necessary when a surrogate is involved. Here is what the progress looks like:
Step 1: Choosing an IVF surrogate
Some intended parents work with friends or family members who volunteer to carry the pregnancy, while others seek a surrogate through agencies or advertising platforms.
An ideal GC is a person who:
Is between 21 and 45 years of age (preferably younger than 35)
Has had at least one (but not more than five) pregnancies
Has had full-term deliveries without complications
Has no more than two C-sections
Maintains a healthy weight and lifestyle (no smoking, alcohol, or recreational drugs)
Has a stable family environment and adequate emotional support to carry the pregnancy
Surrogacy agencies can help simplify the process by screening candidates, managing communication, and navigating the legal and medical logistics.
Before moving forward, intended parents and the IVF surrogate must sign a legal contract clearly defining roles, expectations, and parental rights. The contract should also be reviewed by independent attorneys.
Step 2: Gestational surrogate screening
The surrogate should be medically cleared by the OB/GYN to carry another pregnancy, and this includes confirming whether she has had at least one healthy full-term pregnancy. The procedure involves comprehensive medical, psychological, as well as background screenings, such as:
Reviewing the surrogate’s health history and previous births
Screening for infectious diseases, such as HIV, hepatitis, syphilis, gonorrhea, and chlamydia
Confirming vaccination status for measles, mumps, rubella (MMR), and Tdap (diphtheria, tetanus, and pertussis)
Some clinics may offer legal and psychological counseling to intended parents and the GC, especially in addressing compatibility factors, such as cultural or lifestyle preferences, to ensure a smooth journey.
Ideally, intended parents (or donors) should also undergo genetic carrier screening to ensure they aren’t carriers of any conditions they may pass on to their children. That allows for informed decisions during embryo selection and reduces the risk of chronic health issues in children.
💡Pro tip
Even if you don't have a family history of disease, carrier screening gives you peace of mind. If you find that you’re at a high risk of passing on certain conditions, you can take proactive steps, such as additional embryo testing, to find potentially low-risk options to implant for surrogacy.
You can start with the Nucleus Preview DNA testing kit. It’s one of the most comprehensive tools available for carrier screening, offering clinical-grade testing to analyze your and your partner’s risk for over 2,000 genetic conditions.
Step 3: Preparation and medications for IVF with surrogacy
Once the match is made and the gestational carrier has gone through the screening process, both the egg provider and the GC begin preparing for IVF. Key steps include:
Using hormonal stimulation for the egg provider to develop multiple mature eggs instead of just the one produced in her natural cycle, increasing the chances of retrieving fertilizable eggs.
Preparing the surrogate’s uterine lining using estrogen and progesterone to make the uterus more receptive.
Synchronizing the egg provider’s and surrogate’s cycles for fresh embryo transfer. However, frozen embryos offer more flexibility since they can be safely stored until the uterus is ready.
Sperm quality can also affect fertilization and embryo health, so the sperm provider should prepare by avoiding alcohol, tobacco, and recreational drugs. It’s advisable to avoid heat exposure, such as hot tubs, saunas, and laptops on the lap. Additionally, maintaining a healthy weight, managing stress, and taking male fertility supplements can help.
Step 4: Egg retrieval, fertilization, and preimplantation testing
When the egg provider’s follicles are ready, a fertility specialist retrieves the eggs through a minor outpatient procedure under light sedation. The eggs are combined with the sperm from the intended parent or donor in a lab to create embryos.
The resulting embryos are monitored for development and often given a grade to help with embryo selection. Once embryos are five to six days old, your clinic may recommend preimplantation genetic testing (PGT) to assess embryo health before transfer.
There are several types of PGT screening options, each serving a different purpose:
PGT test | What it does |
|---|---|
PGT-A | Identifies embryos with the correct number of chromosomes, which are more likely to implant and lead to a healthy pregnancy |
PGT-M | Used when one or both parents are carriers of known genetic conditions like cystic fibrosis, hemophilia, or sickle cell disease |
PGT-SR | For carriers of known chromosomal rearrangements, screens for extra or missing chromosomal material. |
PGT-P | Examines multiple genes influencing the risk of complex, late-onset conditions like diabetes, heart disease, or certain cancers |
After PGT, embryos are frozen while awaiting results. Your fertility clinic will receive the report and guide you in selecting the best embryos for transfer.

Bonus reads: Learn more about sex accuracy in PGT-A.
Step 5: Embryo transfer
Once embryos are ready for transfer, one (or sometimes two) is selected and transferred into the surrogate’s uterus. This quick, non-surgical procedure takes about 15 minutes.
The surrogate may be asked to have a full bladder during the process, since it makes the uterus easier to see. Doctors get a clearer ultrasound image as they insert the catheter into the uterus.
After the procedure, the surrogate will rest for 20 to 30 minutes at the clinic. She can resume light daily activities afterward, but should avoid excessive straining for the next 48 hours.
Step 6: Pregnancy testing, monitoring, and delivery
About 9–11 days after embryo transfer, the IVF surrogate takes a blood test to measure the pregnancy hormone (hCG). If the test is positive, hormone support continues, and an early ultrasound is scheduled in 6–7 weeks to confirm the pregnancy (detect a fetal heartbeat).

Source: Mart production
If the pregnancy is viable, the surrogate transitions to routine prenatal care, with ongoing support from the surrogacy agency and the intended parents.
Many families choose to be involved during key appointments and milestones, if the carrier is comfortable with that. Delivery is coordinated with a shared plan, and many intended parents are present in the delivery room or nearby to meet their baby immediately.
Bonus reads: Learn about prenatal genetic testing options in these guides:
Gestational surrogacy success rates
Gestational surrogacy has become increasingly common in the U.S. Between 1999 and 2013, gestational carrier cycles resulted in 13,380 deliveries and the birth of 18,400 babies. Most were single births (64%), followed by twins (34%), and a small percentage were triplets or more (2%).
According to the Society of Assisted Reproductive Technology, the average birth rate for gestational surrogacy is 58.9% per embryo transfer. Success rates vary depending on the age of the mother (egg provider), since egg quality declines over time:
Age of the mother | Average live birth rate |
|---|---|
20–24 | 67.9% |
25–29 | 64.3% |
30–34 | 59.5% |
35–39 | 52.9% |
40–44 | 39.7% |
45–49 | 19.4% |
Success rates are typically higher with egg donors who are young and healthy. The national average live birth rate for gestational surrogacy with donor eggs is 64.7% per transfer.
How much does IVF with a surrogate cost?
IVF with a surrogate comes with significant costs. They typically range from $100,000 to $140,000, but can rise to $250,000 or more, especially if multiple IVF cycles or additional medical support are necessary.
The cost covers anything from legal and agency fees to the surrogate’s compensation and medical care. In some cases, the costs can be higher due to complications, location, or added services like egg and sperm donation, which same-sex couples must consider.
Here is a breakdown of the most common expenses:
Expense | Estimated cost range |
|---|---|
Agency fees | $15,000–$55,000 |
IVF surrogate compensation | $35,000–$95,000 |
Legal fees | $10,000–$25,000 |
IVF and embryo creation | $15,000–$40,000 per cycle |
Medical expenses (prenatal and delivery) | $10,000–$20,000 |
Egg donation (if necessary) | $30,000–$40,000 |
Sperm testing | $1,000–$5,000 |
Travel and accommodation expenses, carrier screening, and preimplantation genetic testing can also increase the overall amount.
Most insurance providers don’t cover surrogacy, but some parts of fertility treatment may be included in your policy, so make sure to check with your provider.
How to improve your chances of having a baby with IVF surrogacy
Given the emotional and financial strain that IVF surrogacy entails, it’s natural that you want it to work the first time. Here are a few ways to boost your chances:
Choosing a clinic with experience in IVF surrogacy
Finding a genetically compatible donor, if necessary
Doing carrier screening
Selecting the best embryo for transfer
Embryologists already use a grading system after preimplantation genetic testing to assess embryo quality. Parents typically have minimal input in the embryo selection process because the grading reports are designed for clinics.
If you’re looking for a more supportive and tailored IVF surrogacy journey, you should explore Nucleus IVF+.
Nucleus is a health, fertility, and genetic testing support platform that can guide you through every stage of the IVF process, from connecting you with the right clinics and donors to bringing you all the necessary tests and tools for selecting the potentially strongest embryo.
How Nucleus IVF+ supports your entire IVF surrogacy journey
Nucleus IVF+ is an all-inclusive package that provides end-to-end support during your IVF journey. Our goal is to make you feel more confident and informed as you navigate the emotionally complex moments and decisions during IVF.
With Nucleus IVF+, you can:
Connect with pre-vetted partner clinics that meet your specific needs.
Access a network of genetically compatible egg or sperm donors to maximize success potential.
Navigate IVF cycles with unlimited support from fertility specialists and genetic counselors at every stage.
Get personalized fertility care with access to fertility consultations and unlimited genetic counseling sessions.
Nucleus IVF+ also gives you access to innovative products like Nucleus Preview and Nucleus Embryo for no additional cost.
Nucleus Preview enables whole-genome carrier screening for over 2,000 genetic disorders that you might unknowingly pass on to your child.
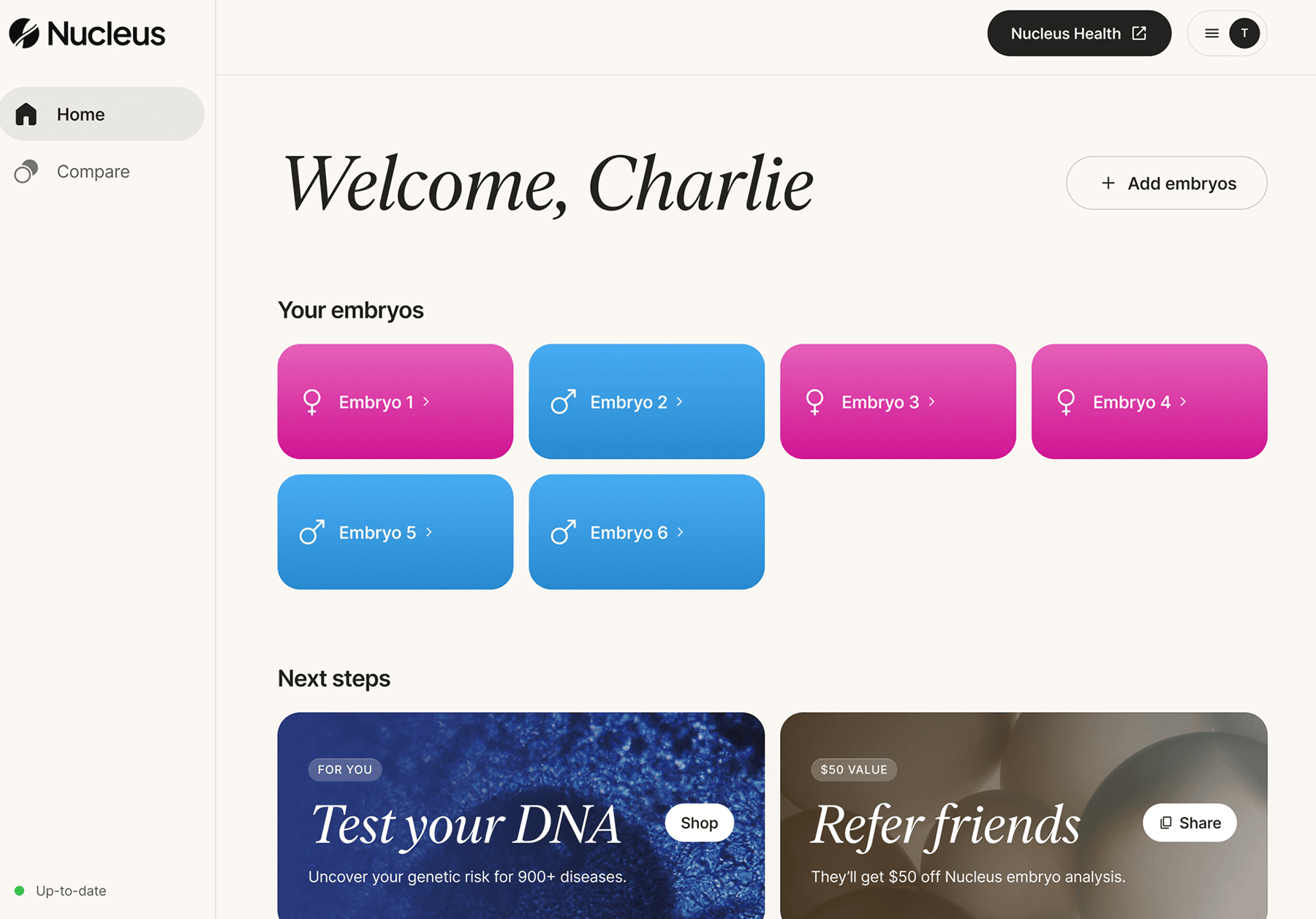
Once you have your embryos created, you can use Nucleus Embryo — the first genetic optimization software of its kind — to explore each embryo’s complex traits, well-being, and long-term health potential over numerous genetic factors.
The platform is designed for parents. You can compare up to 20 embryos on an intuitive dashboard and sort them by features that matter to you, such as the risk for common and rare conditions, like:
Type 2 diabetes
Breast cancer
Alzheimer’s disease
Parkinson’s disease
ADHD
If you’re already halfway through the IVF process, you can opt for the Nucleus Embryo product so you don’t have to pay for the IVF+ bundle.
To start your tailored experience, book an onboarding call with Nucleus experts today.
Note: Nucleus is HIPAA-compliant and maintains the highest standards of privacy and security.
Featured image source: RDNE stock project
















