

In-vitro fertilization, or IVF, helps people conceive by fertilizing an egg with sperm outside the body, then implanting the resulting embryo into the uterus to achieve pregnancy.
The latest reproductive technologies have also made it possible to screen embryos for genetic abnormalities before implantation. This type of proactive testing gives new hope to couples handling infertility, recurrent miscarriage, or inherited genetic conditions.
PGS (Preimplantation Genetic Screening) and PGD (Preimplantation Genetic Diagnosis) are powerful yet distinct approaches to embryo testing.
Understanding the difference between PGS and PGD is more than a technical detail. It can shape the course of treatment and provide greater clinical precision during an emotionally complex process.
This PGS vs. PGD testing guide will:
Break down the science behind each approach
Explore when and why they’re used
Navigate their differences to support informed reproductive decision-making
Note: While PGS and PGD continue to appear in conversations and online forums, current clinical practice refers to these tests with more specific, updated names — mainly PGT-A, PGT-M, and PGT-P.
PGS vs. PGD: An overview
If you’re new to IVF genetic testing, terms like PGS, PGD, and other acronyms can feel overwhelming. So, before comparing them, let’s understand what each test does and how it may impact your IVF journey. The goal is to:
Reduce the risk of misinterpretation
Set realistic expectations based on the results
Find opportunities for more targeted care
What is PGS?
PGS is a genetic test conducted before implantation during the IVF process to evaluate embryos for chromosome abnormalities, specifically looking for errors in the number of chromosomes, known as aneuploidy. The test is now more accurately known as PGT-A — Preimplantation Genetic Testing for Aneuploidy — a name that better reflects its purpose.
PGS/PGT-A’s immediate use case is to ensure that the implanted embryo is euploid — i.e., it has the correct number of chromosomes: 46 in total, with half contributed by the egg and the other half by the sperm. To do this, the test screens the embryo for:
Monosomy: The absence of one chromosome from a pair
Trisomy: The presence of an extra chromosome in a pair
Segmental aneuploidy: Missing or extra pieces of chromosomes above a certain size threshold

Source: Mikhail Nilov
There are also more advanced PGS options that can detect a broader range of chromosome abnormalities beyond standard aneuploidy, such as:
Triploidy: Three copies of each chromosome
Mosaicism: Some cells in the embryo have a normal number of chromosomes, while others don’t
Uniparental disomy: Both copies of a chromosome come from one parent instead of one from each
One of the more expansive and advanced testing options today is PGT-P, which screens multiple genes to assess an embryo’s genetic risk for common diseases like heart disease, cancer, and diabetes.
Note that PGS cannot correct chromosome abnormalities in the embryo — it only detects them. It also doesn’t guarantee implantation or live birth.
What it can do is help select embryos with the highest likelihood of success, since having the wrong number of chromosomes can lead to failed implantation, miscarriage, or genetic disorders. One 2024 cohort study found that embryos screened with PGS had higher implantation rates (79.8%) compared to those that weren’t screened (63.2%).
What is PGD?
PGD is a type of genetic testing performed during IVF to screen embryos for specific genetic conditions. This test is usually performed when there is a known genetic disorder in the family or when one or both parents carry a detrimental genetic variant that could be passed on to their children.
PGD can only test for monogenic disorders — conditions caused by a change in a single gene. That’s why PGD is now primarily referred to as PGT-M — Preimplantation Genetic Testing for Monogenic Disorders — which clarifies its role in the broader preimplantation genetic testing context.
The goal of PGD is to identify embryos that are free of specific inherited genetic conditions, allowing parents to select those with the highest chance of being healthy. This, in turn, reduces the risk of passing on a genetic disorder to their child(ren).

Source: Vanessa Loring
PGD vs. PGS: 6 differences that set them apart
At their core, PGD and PGS share the same goal — improving the chances of a successful, healthy pregnancy. Still, they differ in key areas, including:
Scope of genetic testing
Ideal candidates
Procedure or testing design
Testing timeline
Costs
Success rates
These fundamental distinctions may help you choose the right test for your IVF journey. Here’s how:
1. Scope of genetic testing
When it comes to identifying genetic conditions in embryos, the capabilities of PGS and PGD differ significantly.
PGS is limited to detecting large-scale chromosomal abnormalities. While it may incidentally identify a handful of major conditions caused by extra or missing chromosomes, such as Down syndrome, Turner syndrome, or trisomy 18, it doesn’t test for specific genetic diseases or inherited monogenic disorders.
PGD, by contrast, is designed specifically to screen embryos for monogenic disorders. In theory, PGD can screen for any monogenic condition, provided that these three conditions are met:
The disease-causing gene is clearly identified
An accurate genetic test can be developed
The condition meets established clinical and ethical guidelines for monogenic testing
This distinction is important if prospective parents decide they need the precision of PGD over the broader screening in PGS.
Here’s a table of the genetic conditions that PGD commonly tests for, grouped by inheritance type:
Inheritance type | Explanation | Examples of genetic conditions |
Autosomal recessive | Disease occurs only if both parents pass on an altered gene copy |
|
Autosomal dominant | Only one altered gene copy is needed to cause the disease |
|
X-linked | Disease-causing gene is on the X chromosome, typically affecting males |
|
2. Ideal candidates
Understanding who stands to benefit most from each type of testing can help guide clinical decisions and patient counseling.
Fertility specialists usually recommend PGS when chromosomal abnormalities are likely to impact embryo viability or pregnancy outcomes. This applies to individuals who:
Are of advanced maternal age (35 and above): The risk of chromosome aneuploidy rises with age, from about 17% under age 35 to around 80% at age 43 and above.
Have experienced recurrent pregnancy loss: Embryos with aneuploidy are a leading cause of miscarriage, affecting half to two-thirds of early pregnancy losses.
Have gone through multiple failed IVF cycles or transfers: PGS can improve the selection of the healthiest embryos.
Have a history of a chromosomally abnormal pregnancy or child: PGS may reduce the recurrence risk.
For the above candidates, the goal of PGS is to increase the chances of a successful pregnancy.

Source: Pavel Danilyuk
As for PGD, the couples that opt for this test usually have no trouble conceiving. They’re more concerned about passing on specific genetic conditions. Ideal PGD candidates are:
Prospective parents with genetic disorders
Carriers of genetic disorders who might be healthy themselves
Individuals with a family history of genetic conditions
Advice 💚
Remember that parents can also be silent carriers—i.e., they carry a genetic variant without showing symptoms of the condition. One of the best ways to identify these carriers is through broad preconception carrier screening—which can be done before or during IVF.
Nucleus offers the most advanced carrier screening options with its Nucleus Preview product. The at-home DNA test leverages whole-genome sequencing technology to analyze ~100% of your genes, which makes it more likely to uncover any new or rare genetic variants you may carry and plan tests for the same.
Nucleus screens for [NUM_CONDITIONS_SCREENED]+ genetic conditions with 99.9% accuracy. You get both — insights into your personal health, as well as comprehensive data to shape your embryo testing decisions. Order your Nucleus Preview kit to get started!
Bonus reads: Learn about these specialized carrier screening tests:
3. Procedure or testing design
PGD, PGS, and other types of preimplantation genetic testing all require IVF as part of the process. In both PGD and PGS, a small number of cells — usually five to 10 — are removed from the embryo for genetic analysis. However, the approach to the analysis differs based on the specific purpose of the test and the type of genetic information being evaluated.
PGS usually calls for basic chromosomal analysis to check for abnormalities — essentially, to count the number of chromosomes and look for large missing or extra pieces. PGD, in contrast, typically employs more advanced techniques like multiplex PCR (polymerase chain reaction). This method amplifies multiple regions of the genome simultaneously, enabling the identification of specific genetic variants within the embryo.
PGD might also prolong the genetic testing process, requiring family members to be tested for known genetic conditions to help the lab isolate family-specific genetic markers.
Source: RDNE Stock project
4. Testing timeline
Both PGS and PGD are integrated into the overall IVF process — they happen after fertilizing the eggs but before transferring the embryo. Still, the exact IVF timeline with genetic testing involved will differ depending on the scope of the test.
The table below should help you understand how the timelines for PGS and PGD compare, along with any potential procedural differences.
Phase | PGS | PGD |
Initial planning | Prior to starting the IVF cycle as the parents’ DNA samples might be required | Well in advance of the IVF cycle to allow enough time for genetic counseling and collecting DNA samples from the aspiring parents and possibly their family members |
Test development | Not required for PGS | Custom test development needed, which can take six to 12 weeks |
IVF cycle and embryo creation | Eggs are retrieved, fertilized, and embryos cultured until day 5 or 6 (blastocyst stage) | No major differences |
Embryo biopsy | Performed during the blastocyst stage, with embryos frozen immediately after | No major differences |
PGT analysis | Basic chromosomal analysis, analysis for rare diseases, and analysis for chronic and late-onset diseases — besides PGT-A, you can also go for modern PGT-P tests that analyzes various common genetic variants to predict the risk of complex diseases like diabetes and cancers | Analysis involves custom testing and genetic markers — you need to go for PGT-M testing to detect mutations caused by a single gene |
Result notification | Results available in seven to 10 days after biopsy | Results take 2–3 weeks, with additional time for complex cases |
Frozen embryo transfer | Scheduled after receiving genetic test results and selecting healthy embryos | No major differences |
Essentially, PGD usually takes longer than PGS — from roughly three weeks to three months — due to additional steps involved in customizing the genetic test for the parent.
Bonus read: Dive into the complete timeline and learn how long PGS testing takes.
5. Costs
On average, PGS costs between $3,000 and $6,000 per IVF cycle, depending on the number of embryos tested and the laboratory used. In contrast, PGD costs run between $7,000 and $12,000 per cycle, reflecting the extra customization and family-specific test development required. These figures cover the biopsy and genetic analysis but not the base IVF cycle costs, which can cost up to $25,000.
Although the upfront costs for PGS and PGD can feel substantial, many patients find they ultimately save time and even additional treatment expenses by avoiding repeated failed transfers.

Source: MART PRODUCTION
6. Success rates
Some prospective parents choose to perform both PGS and PGD analyses to maximize their chances of a healthy pregnancy.
Still, PGS or PGD, even when used together, cannot guarantee a 100% successful and healthy pregnancy, due to inherent limitations.
For instance, PGS reduces miscarriage risk by identifying embryos with normal chromosomes but doesn’t eliminate the chance of miscarriage. Plus, there’s always the possibility of false positives — which could lead to discarding a viable embryo, and false negatives — leading to the transfer of an embryo with undetected chromosome abnormalities.
PGD also doesn’t guarantee 100% accuracy for a few reasons:
Genetic complexity: Many monogenic disorders involve multiple gene variants or unpredictable gene interactions.
Limited detection of chronic or late-onset diseases: Unless a specific gene variant is being tested, PGD and PGS don’t detect variants for chronic or late-onset diseases like heart conditions and cancer.
Limitations in current technology: More complex conditions may not be detectable with standard PGT analysis.
To reduce these uncertainties, many prospective parents choose to add a more thorough genetic analysis to their journey, using genetic optimization software alongside IVF to compare embryos based on their comprehensive genetic profiles.
If you wish to explore genetic optimization, one of the most accessible options you have is Nucleus Embryo.
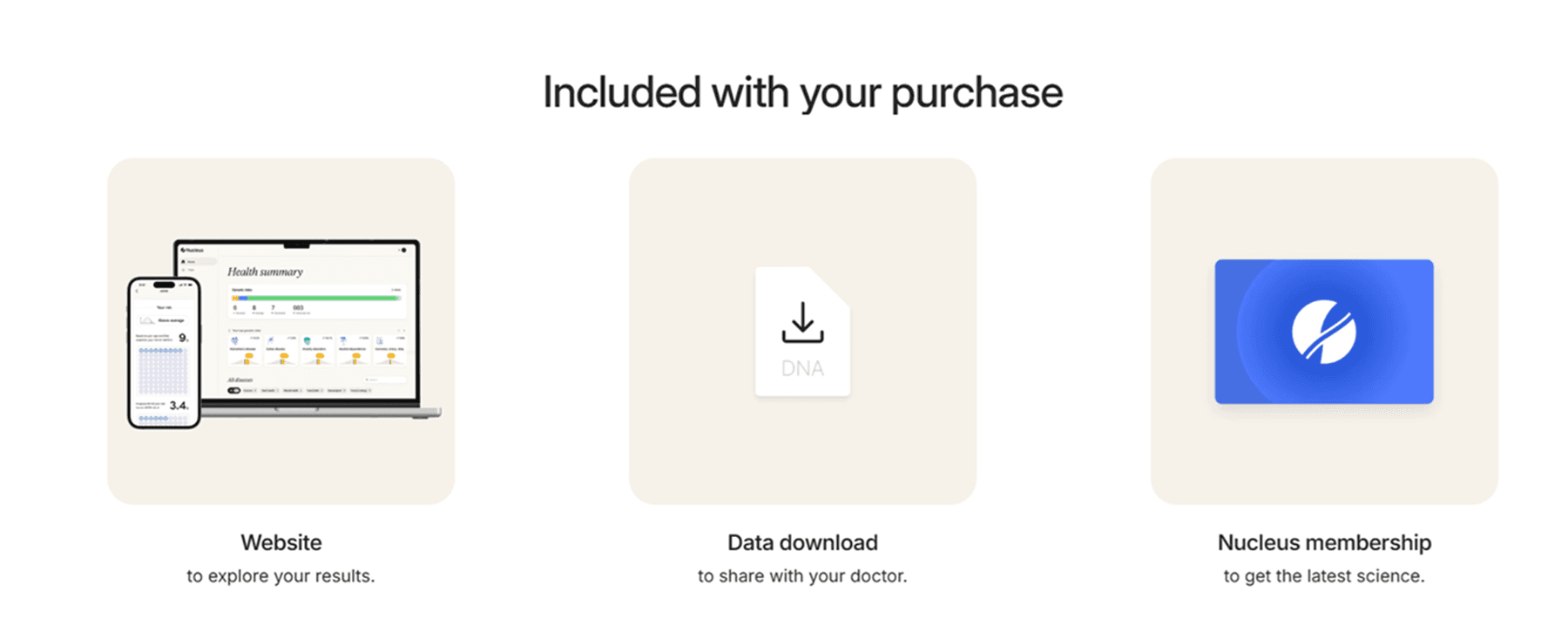
Get comprehensive testing with Nucleus IVF+
Nucleus IVF+ is an all-in-one program that offers concierge support for your entire IVF journey. You can access:
Matching services with top vetted IVF clinics
One IVF cycle
Medications
STD & AMH testing
ICSI included with cycle
Donor selection support
Personal carrier screening tests
PGT testing
Embryo analysis and genetic optimization software
All consultations during treatment — and more.
Nucleus IVF+ comes with numerous solutions, including Nucleus Preview and Nucleus Embryo, to guide your choices during IVF+.
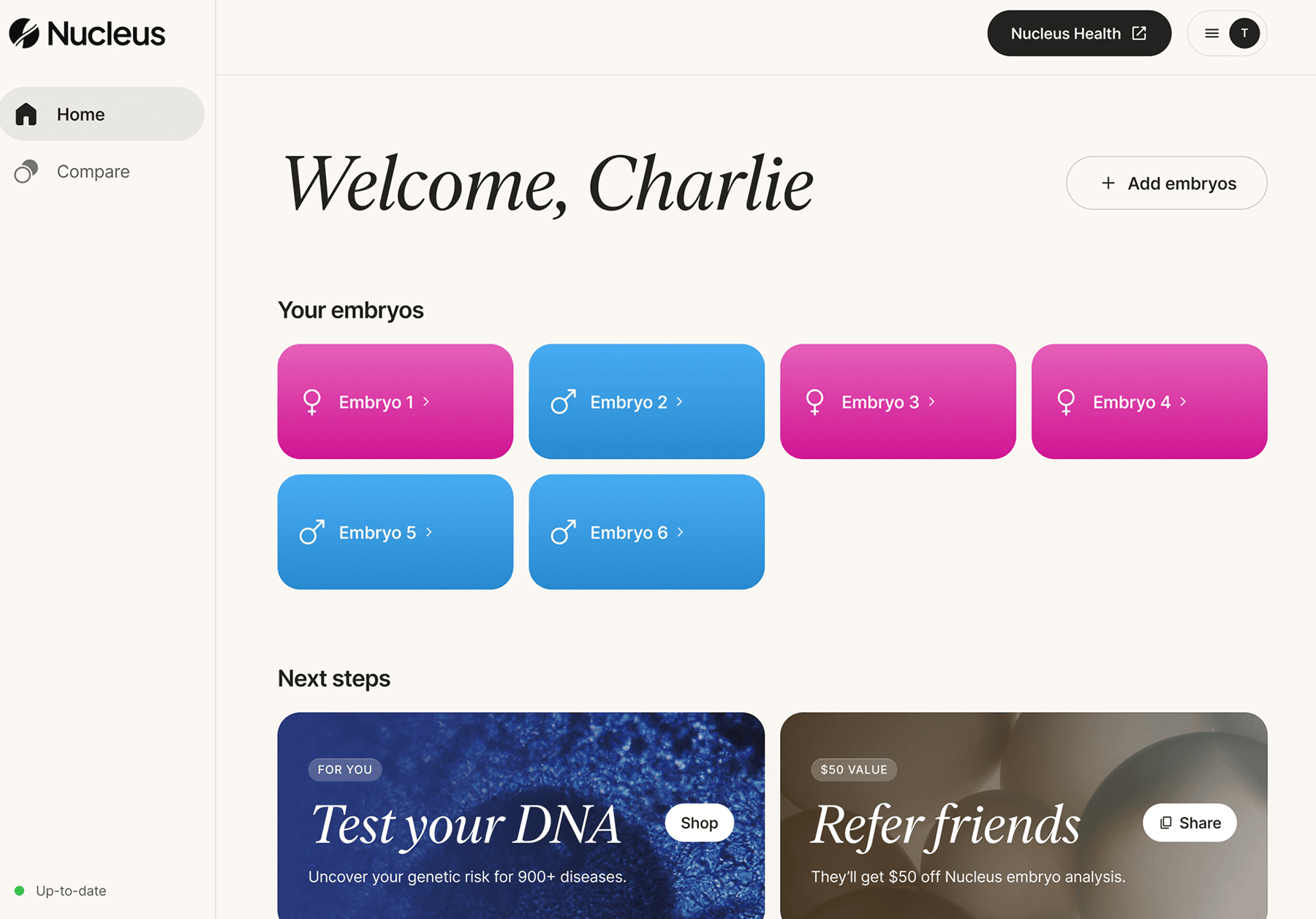
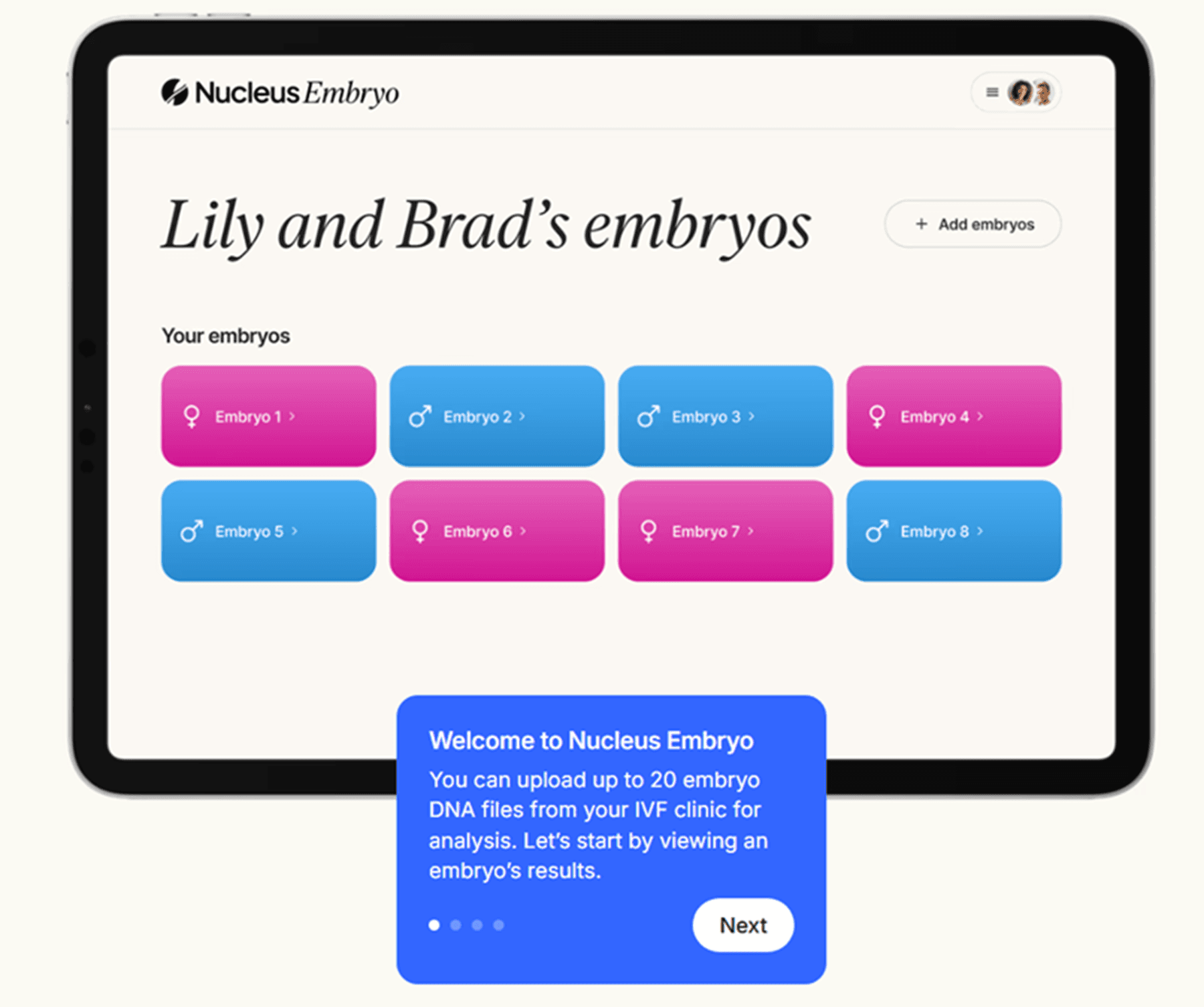
Nucleus Embryo is a first-of-its-kind genetic optimization software designed for IVF couples who want to analyze and compare their embryos with greater clarity. This gives you a common denominator to compare and helps you make one of life’s biggest decisions with confidence and compassion.
Nucleus can reveal embryo insights under three broad categories, along with analyses for a wide selection of traits and conditions for each embryo:
Health conditions: Heart disease, cancer risk, ADHD, depression, and dozens of hereditary disorders, including rare conditions like cystic fibrosis and hemochromatosis
Physical traits: Includes eye color, height, hair color, and male-pattern baldness
Well-being and mental health: Psychiatric conditions and other neurological traits
Want to explore the service first? You can answer a few questions here to get started.

Backed by science, guided by love: Leveraging Nucleus for decisions
Nucleus adds a final, personalized layer of understanding to your IVF journey so you can make informed, responsible decisions based on what matters most to you.
While this comprehensive analysis is made possible by rigorous, peer-reviewed science, the results are designed for you — not the scientists. We translate complex genetic data into clear, relatable insights, putting everything in one place so you can compare embryos side by side.
While similar services may offer a limited range of decision points or one-time consultations, Nucleus gives you an interactive platform where you can interpret results and make choices at your own pace and without judgment. You can sort, compare, and even name your embryos before choosing one for implantation.
You’ve already taken so many brave steps. Now, let Nucleus guide you toward the future you’re building. Book a consultation with our experts to get started.
The platform is HIPAA compliant and adheres to robust data protection practices.
You may also like…
Here are some more family planning guides you can go through:
Featured image source: Kelly Sikkema










